Today Claire and I journey to Memorial Sloan-Kettering Cancer Center in Manhattan, for our second-opinion consultation with Dr. Carol Portlock, the lymphoma specialist I saw back in January. “Second opinion” may be something of a misnomer in this case, because we’re actually seeing her first this time – although, as before, it’s turning out to be a collaborative process between the two doctors, a team approach.
Today Claire and I journey to Memorial Sloan-Kettering Cancer Center in Manhattan, for our second-opinion consultation with Dr. Carol Portlock, the lymphoma specialist I saw back in January. “Second opinion” may be something of a misnomer in this case, because we’re actually seeing her first this time – although, as before, it’s turning out to be a collaborative process between the two doctors, a team approach.Getting to the hospital takes some doing. We’re driving, once again - to avoid the logistical difficulty of carrying the large envelopes of CT and PET scan films on train and subway. City traffic turns out to be heavier than it was last time. As we get to the hospital, we find a half-block line of cars waiting to get into the parking garage. After five minutes or so of sitting in that line (which is going nowhere fast), it occurs to me that we don’t both need to be in the car. I get out – the large envelopes of films under my arm – and Claire switches over to the driver’s seat, to finish waiting for a space to open up in the parking garage. I walk into the building, find my way upstairs, and get the films to the receptionist. I'm just five minutes late for our appointment (getting the scans to the Sloan-Kettering staff early is the most important thing, because the entire day’s schedule hangs on their interpretation by some nameless radiologist on the staff).
After check-in, I sit down in the waiting area. Claire joins me a half-hour or so later. We wait for maybe a half-hour longer, before a nurse has me come in for a quick vital-signs check. More waiting, then we’re invited back in again, so a resident (a doctor-in-training) can examine me. We sit in the examining room for maybe half an hour longer, before Dr. Portlock finally comes in – about two hours after my scheduled appointment time. The wait doesn’t really bother us, though, because we’re most concerned that everything be done right. Take your time, O mystery radiologist – what you see in those scans will make a huge difference in my life.
I’ve determined ahead of time that I have four basic questions for Dr. Portlock. I’m calling them, for memory purposes, “the 4 Rs” – remission, radiation, Rituxan and right lung:
Remission: Does the PET scan report indicate that I am, indeed, in remission?
Radiation: Are radiation treatments advisable?
Rituxan: Would a course of maintenance treatments with Rituxan help prevent the cancer’s return?
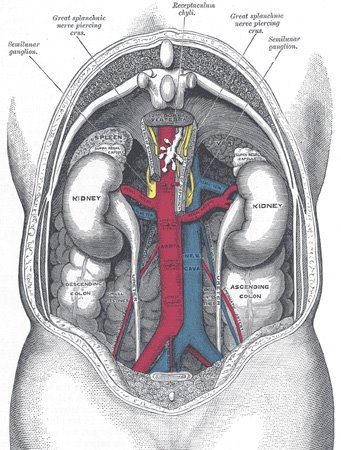
Right Lung: Earlier scans have flagged a small growth – a “nodular density” – in one of my lungs, as a possible area of concern. The most recent PET scan shows that this area has increased in size since the last scan – although it didn't light up on the scan as any kind of malignancy. I want to be sure to ask the doctor what she thinks this is.
Dr. Portlock accurately sums up the details of my situation. She describes how the chemo treatments have shrunk the abdominal tumor, and how the PET scan has confirmed that only scar tissue remains. Eventually, she says, the mass will get even smaller, collapsing in upon itself.
I ask her my questions...
 Remission: YES, she says, the PET scan indicates that I am in remission. (Hooray!)
Remission: YES, she says, the PET scan indicates that I am in remission. (Hooray!)Radiation: On the question of radiation, her answer is NO. In my case, the possible side-effects of radiation outweigh the advantages. Given the location of the mass, and the fact that (due to my comparatively large body size) I would need a heavy radiation regimen, the side effects would likely be quite severe. Because lymphoma is a systemic – rather than a localized – disorder, radiating what remains of the abdominal tumor could help prevent any relapse in that particular area, but will do nothing for the rest of the lymphatic system. Were I to have a recurrence of cancer, it could happen anywhere in that system – so Dr. Portlock sees no advantage of targeting the spectral remains of my tumor. She recommends that we go into a watch-and-wait mode, and that I be monitored with CT scans every three or four months for a year, then less frequently after that. If there’s a relapse, radiation could be considered at that time, as one treatment option among several.
 Rituxan: As for maintenance treatments with Rituxan, Dr. Portlock’s answer is NO. Her view is that long-term treatments with Rituxan would be of uncertain benefit in my situation. Furthermore, there’s a possibility that long-term use of this drug – which seeks out and destroys healthy B cells, as well as cancerous ones – could eventually depress my immune system. In the event of a relapse, she says, I will need a strong immune system, so she wants to use this powerful medicine only when there are clearly malignant cells that need to be targeted.
Rituxan: As for maintenance treatments with Rituxan, Dr. Portlock’s answer is NO. Her view is that long-term treatments with Rituxan would be of uncertain benefit in my situation. Furthermore, there’s a possibility that long-term use of this drug – which seeks out and destroys healthy B cells, as well as cancerous ones – could eventually depress my immune system. In the event of a relapse, she says, I will need a strong immune system, so she wants to use this powerful medicine only when there are clearly malignant cells that need to be targeted. Right Lung: I ask her about the nodule in my lung, and she says it does not appear, from the PET scan, to be malignant. Even so, she recommends I talk with Dr. Lerner about getting it checked out by a pulmonologist or a thoracic surgeon. If it looks suspicious, it would be possible to do a needle biopsy and find out for sure. Because of the clean PET scan, though, she thinks it is most likely a harmless growth of some kind.
Right Lung: I ask her about the nodule in my lung, and she says it does not appear, from the PET scan, to be malignant. Even so, she recommends I talk with Dr. Lerner about getting it checked out by a pulmonologist or a thoracic surgeon. If it looks suspicious, it would be possible to do a needle biopsy and find out for sure. Because of the clean PET scan, though, she thinks it is most likely a harmless growth of some kind.We thank Dr. Portlock and head down for a late lunch in the hospital cafeteria, before fetching the car and heading for home. Claire and I agree that, after all the recent talk about radiation treatments lasting well into the summer, the word “remission” still doesn’t sound quite real to us. If, after talking with Dr. Portlock, Dr. Lerner concurs with this assessment, we’ll begin to breath a sigh of relief at last.